

Antidepressants are the fastest growing class of psychotropic drugs: there are not only new drugs, but also whole generations of antidepressants with new mechanisms of action.
Currently, three mechanisms of action of antidepressants are established:
effect on the reuptake of monoamines - reverse selective inhibitors of neuronal serotonin reuptake (SSRI) and selective
inhibitors of reverse neuronal uptake of noradrenaline (NARI);
monoamine oxidase inhibition (reversible and irreversible MAO inhibitors);
blockade of monoaminergic receptors.
It is believed that affective disorders are associated with a violation of a number of neurotransmitter systems, among which the main place belongs to the violation of serotonin transport and the activity of 5-HT2C platelet receptors.
General properties of Zoloft
A common property of selective serotonin reuptake inhibitors is the inhibition of serotonin re-entry from the synaptic cleft into the presynaptic neuron without a noticeable effect on the delivery of other transmitter substances.
Fluoxetine , fluvoxamine belong to the SSRI of a monocyclic structure ; to bicyclic - Zoloft , paroxetine and citalopram . It is considered that bicyclic SSRIs are superior to monocyclic in such parameters as selectivity and severity of action.
Numerous scientific studies of this group of drugs, including comparisons made with tricyclic antidepressants (TCAs), traditionally used in psychiatry in the treatment of depression (amitriptyline, imipramine , clomipramine , etc.), have shown their high therapeutic efficacy, comparable to tricyclic compounds, but with fewer side effects. However, it was found that, despite belonging to one group of chemical compounds, the spectrum of antidepressant activity of each of them has its own characteristics, which determine the preferential indications for individual use and deserve undoubted attention.
Clinical effect of SSRIs
The ability to influence the depth of a vitally modified affect is one of the most important properties of a modern antidepressant. According to S.N. Mosolov, with severe endogenous depressions, the clinical effect of SSRIs, compared to TCAs, develops somewhat slower (by the 4th week), but by the end of the 2nd month of treatment is comparable to tricyclic antidepressants. To cancel the drug group SSRIs after several weeks of treatment due to lack of effect is impractical, it should come a little later.
Of greatest interest to clinicians are the so-called atypical depression, for which, according to modern classifications, the following features are characteristic:
increased appetite until hyperphagia ;
weight gain;
hypersomnia ;
situationally motivated nature of the mood and its dysphoric hue;
general weakness, lethargy;
heightened sensitivity to situations of frustration;
reverse nature of daily mood swings.
Of interest is another disorder, dysthymic , with SSRIs exhibiting high therapeutic efficacy. For dysthymic disorder is characterized by depressed mood during the day in conjunction with subjective complaints, lasting at least two years. During this period, two or more of the following symptoms are usually observed: loss of appetite or overeating, insomnia or hypersomnia , decreased energy or fatigue, low self-esteem, difficulty concentrating and making decisions, a sense of hopelessness.
Such patients are very resistant to therapy. However, according to S.N. Mosolov, in 53.8% of cases, patients respond positively to SSRI therapy, whereas for TCA this figure is only 41.2%.
When approaching the treatment of depression as a chronic recurrent disease, three main stages or stages of therapy can be distinguished:
cupping;
treatment or stabilizing (6-9 months);
prophylactic (supportive).
Recurrences of recurrent depression within two years after the end of active or stabilizing therapy develop in 50-75% of patients. Without pharmacological prophylaxis - 70-80% of patients who have had three depressive episodes and more than three years, usually develop a relapse. According to the WHO, antidepressant treatment should be continued for 12 months after the disappearance of the acute symptoms of depression.
Prophylactic therapy
Patients with relapses of depression during the last five years of the disease need preventive therapy. The question of stopping thymoanaleptic therapy can be raised only after a 2-year euthymic period.
Speaking about the advantages of SSRIs, it should be emphasized that, unlike TCAs, they are safer for patients with intercurrent somatic diseases, such as prostate adenoma, angle - closure glaucoma, cardiovascular diseases, obesity, and others.
SSRIs are combined with other drugs ( antihypertensives , b-blockers, antacids, antihistamine and oral contraceptives), psychotropic (neuroleptics, tranquilizers). They do not interact with tyramine and alcohol. Indications for use of SSRIs are:
recurrent depression (major depressive episode);
bipolar depression (in combination with timoizoleptiki );
dysthymia; - obsessive- compulsive disorder.
According to many authors, the relative indications for SSRIs are panic disorder, bulimia, social phobia, alcoholism and other substance abuse, chronic pain syndromes, mixed anxiety-depressive states, somatoform disorders. Zoloft ( sertraline ) is a bicyclic drug, naphthylamine derivative is a powerful selective serotonin reuptake inhibitor, it does not cause blockade of muscarinic , serotonin, adrenergic and GABA- ergic receptors. Therefore, the drug has virtually no anticholinergic , cardiotoxic and sedative properties. The pharmacokinetic characteristics of Zoloft seem to accumulate the positive properties of the whole group of antidepressants. The concentration of the drug in the blood is reached after 6-8 hours after administration. Plasma protein binding - 98%. Zoloft is actively metabolized in the liver, but has no active metabolites. The half-life of the drug from blood plasma is about 26 hours, and its demethylated metabolite is 62-109 hours. The resulting metabolites are excreted in the urine and feces in equal proportions, a small part of the drug - unchanged in the urine. The equilibrium concentration of the drug in the blood is established in a week.
Timoanaleptic actions
The profile of psychotropic activity is based on a distinct thymoanaleptic effect with a weak stimulating component. Although the first signs of improvement appear already in the 1st week of therapy, 3-4 weeks are needed to achieve an obvious effect, and sometimes 6-8 weeks. The effect increases as treatment continues.,
Zoloft is used to treat all types of depression of varying severity. Despite the almost complete absence of sedation, sertraline has a positive effect in patients with anxiety depressions and sleep disorders, anxiety reduction occurs much faster than using fluoxetine . In the case of a mixed anxious and melantial affect, the vital manifestations are reduced in parallel, followed by a normal mood, an increase in mental activity occurs, suicidal thoughts and somatoform disorders disappear .
In small doses (up to 100 mg per day) the drug is used as a preventive measure for recurrent depressions. At the same time, the number of relapses decreases (compared to placebo) by 30%. According to some reports, the drug is especially effective for somatized and atypical depressions with bulimia and an increase in body weight. In addition, sertraline is used to treat obsessive- phobic disorders. In these cases, the best effect is achieved with the appointment of 150-200 mg of the drug per day for 8-12 weeks.
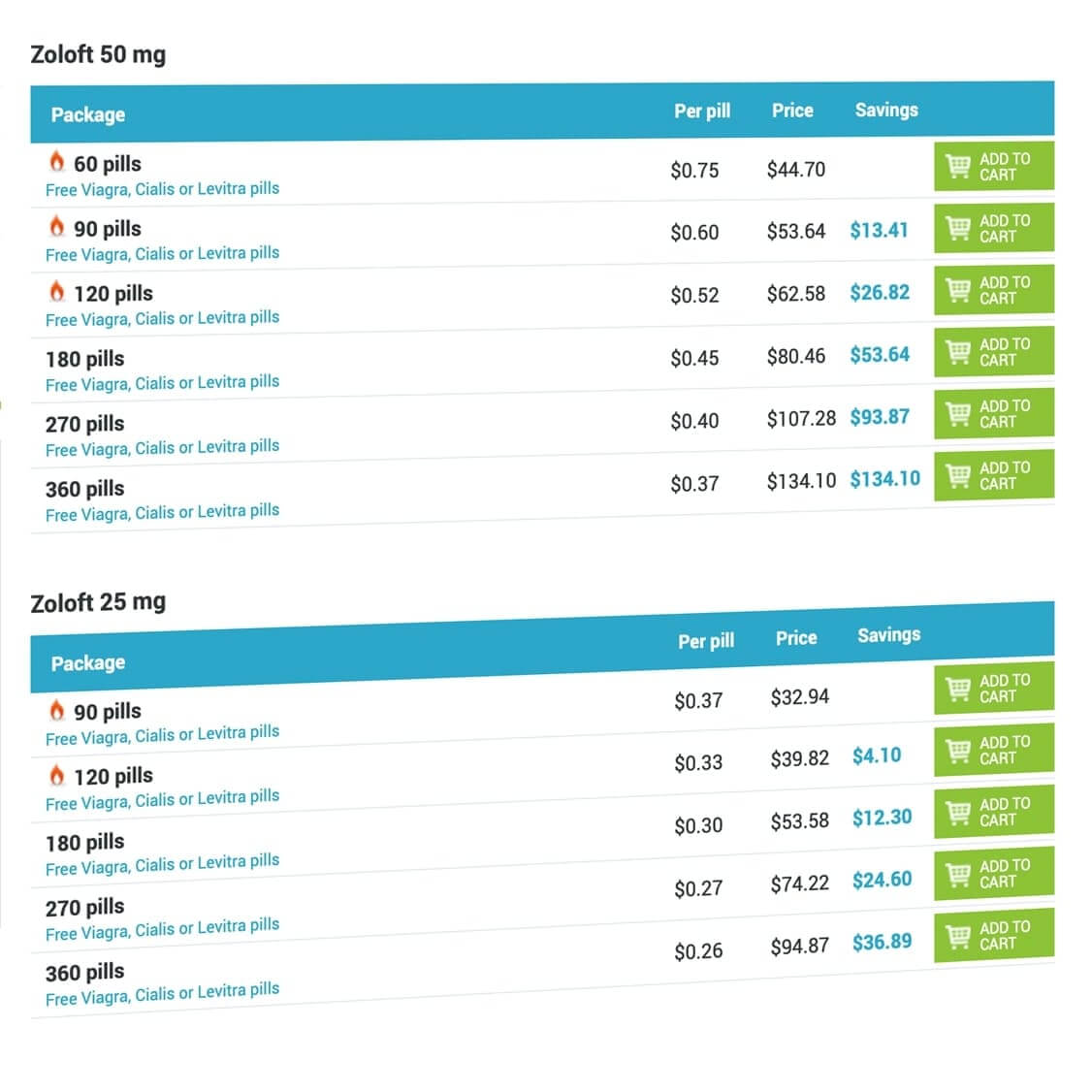
Since the half-life of the drug is about a day, it will be applied in a single dose - 50-200 mg / day (the minimum and optimal dose is 50 mg). If necessary, the dose is increased by 50 mg / day 1 time per week. For prophylactic purposes, 50-100 mg per day is enough.
Zoloft is effective and safe for all age groups: children, adults and elderly patients. The uniqueness of the drug lies in the fact that individual selection of the dose, depending on age, is not required.
And overdose
Zoloft is highly safe in case of accidental or deliberate overdose (even 160 daily doses do not cause death). The drug does not enhance the effect of alcohol, carbamazepine , haloperidol on cognitive and psychomotor functions while taking it. Sertralin does not cause sedation and does not affect the psychomotor function, does not cause dependence, does not possess a cardiotoxic effect, is well tolerated by patients with cardiovascular diseases. Proved high efficacy of the drug for obsessive- compulsive and panic disorders, generalized anxiety. It is also effective in resistant forms of depression in patients treated with TCA.
It should be emphasized that Zoloft can be used effectively with tricyclic antidepressants in small dosages. With long-term use Zoloft does not increase tolerance and does not develop dependence. The sudden withdrawal of the drug does not lead, in contrast to other SSRIs, to the development of specific somatic and psychopathological symptoms. Currently, Zoloft is widely and effectively used in premenstrual tension syndrome, as well as in the treatment of premature ejaculation in men. The use of Zoloft during pregnancy and breastfeeding is possible when the expected benefit outweighs the possible risk. In the literature, there is evidence of the effective use of Zoloft in the combination therapy of schizophrenia in the presence of negative symptoms, depression, obsessive- compulsive disorders. The best effect is achieved in combination with atypical antipsychotics.
Contraindications
When taking Zoloft can experience undesirable reactions: dry mouth, excessive sweating, dizziness, tremor, diarrhea, dyspepsia, nausea, anorexia, insomnia, drowsiness, impaired sexual function (mainly - delayed ejaculation). In Bennie et al study, the following performance indicators sertraline and fluoxetine in the treatment of 248 patients with major depressive disorder (MDD) sertraline efficiency - 59%, fluoxetine - 51%. However, with a differentiated analysis of effectiveness with regard to various variants of depressive disorder, significant differences between the studied antidepressants were revealed. Sertralin was more effective than fluoxetine in the treatment of patients with melancholic depression (59% versus 44%), severe MDD (59% versus 41%) and with severe psychomotor agitation (62% versus 39%). Dr. Nutt suggests that these differences are due to the activating effect of fluoxetine on 5-HT2C receptors, although some researchers explain them by agonism sertraline to s-receptors. As evidence of his suggestion, Dr. Nutt cites indicators of the frequency of premature discontinuation of therapy due to an activating side effect: among patients who participated in the study, premature discontinuation of therapy in 5.6% of cases was associated with fluoxetine and only 2.8% - sertraline .
Additional confirmation of the importance of the activation of 5-HT2C receptors was obtained in the Small study when comparing fluoxetine and placebo with four degrees of severity of agitation. In the absence of signs of agitation at the time of initiation of therapy, fluoxetine administration was accompanied by a significantly more pronounced reduction in HAM-D indicators than placebo treatment. In cases of severe agitation, the effectiveness of fluoxetine was lower than the placebo effect. These data prove that the activating effect of fluoxetine on 5-НТ2С-receptors can negatively affect the results of treatment of certain subtypes of MDD. Bisserbe et al. (1996) provide comparable data from 6-week treatment for 81 patients. Dr. Nutt notes that the results of these studies suggest that agitation is a predictor of the low efficacy of fluoxetine and the relatively more pronounced therapeutic effect of sertraline .
Significant differences are also found between sertraline and paroxetine . Zanardi and colleagues compared the effectiveness of these drugs in the treatment of psychotic depression. The authors found that in the sertraline group, treatment efficacy was much higher (75% versus 27%), which was partly due to differences in the frequency of premature discontinuation of therapy: 40% in the paroxetine group and not a single case in the sertraline group . According to Dr. Nutt , these differences are due to two factors: the activating effect of sertraline on s-receptors and its effect on dopaminergic systems.
Symptoms
To compare sertraline and fluoxetine , Dr. Nutt turned to an analysis of the symptoms of depressive disorders. In accordance with the accumulated clinical experience, there is no doubt that the activating effect of fluoxetine leads to considerable difficulties in the treatment of some patients with severe anxiety associated with MDD. In comparing the effectiveness of sertraline and fluoxetine in the treatment of patients reveals that sertraline provides a more pronounced reduction of anxiety than fluoxetine (Sechter et al., 1993). These data support the suggestion that fluoxetine may cause the development of alarming symptoms.
SSRIs vary in effect on sleep function. Reliable evidence has been obtained that nighttime awakenings and the number of slow waves in sleep cycles are associated with 5-HT receptor activity. According to Sechter , after 24 weeks of therapy for patients with early insomnia sertraline provides a reduction of the 4th point of the HAM-D scale to 0 points (ie, a complete reduction of early insomnia ) in 47.4% of cases, and fluoxetine in 36.5%. Bisserbe et al. (1996) confirm that sertraline is more effective than fluoxetine for sleep disorders in depression. According to Dr. Nutt , these differences may be related to the activating effect of fluoxetine on 5-HT2C receptors, since the data obtained by the authors are consistent with the results of biological studies, namely:
Provocation with the introduction of mCPP activating 5-HT2C receptors leads to a reduction in the total sleep time and an increase in the number of nighttime awakenings. Moreover, patients taking sertraline subjectively appreciate sleep quality more highly than patients receiving fluoxetine.
SSRIs affect body weight in different ways. It is known that patients with depression, especially severe, lose weight significantly, so it is important to choose an antidepressant that does not cause weight loss. According to Bisserbe , after a week of sertraline therapy, the patient's body weight (mass index on the HAM-D scale) returns to normal, while fluoxetine is accompanied by an even greater decrease in body weight. Dr. Nutt suggested that these data are also explained by the activating effect of fluoxetine on 5-HT2C receptors and determine the contraindications for the administration of fluoxetine in such patients.
Cognitive impairment
Depression is often accompanied by severe cognitive impairment - decreased concentration and memory impairment. Virtually all antidepressants improve cognitive function in patients with depression. Tricyclic drugs, due to their side effects, are less effective against cognitive impairment than SSRIs. Linden and co-authors performed a comparative study of sertraline and fluoxetine in the treatment of elderly patients with an assessment of cognitive functions using a numeric character replacement test. Against the background of sertraline therapy, his results improved, and fluoxetine was accompanied by only a slight positive trend. The latter, apparently, can also be explained by the activation of 5-НТ2С receptors during therapy with fluoxetine .
Evidence of SSRI differences in the effectiveness of long-term therapy was obtained as a result of four large comparative studies of fluoxetine and sertraline using strict criteria for evaluating effectiveness. According to Van Moffaert et al., On the 8th week of treatment, about 12% of patients in both groups ( sertraline and fluoxetine ) were assessed as clinically normal - 1 point on the CGI scale “severity of the condition”. The continuation of therapy was accompanied by an increase in the differences between the drugs: by the 24th week, the clinical rate was detected in 50% of patients from the sertraline group and about 35% from the fluoxetine group ; by week 32, these figures were 60% and 38%, respectively. The advantage of sertraline over fluoxetine during long-term treatment of depression was confirmed by data from a 24-week study by Sechter et al. (1993). The presented results suggest that sertraline is preferable to fluoxetine as a means of long-term treatment of BDR .
Thus, the possibility of widespread use of Zoloft in the treatment of depression is due to:
high efficacy (antidepressant effect is comparable to the effectiveness of classical antidepressants);
good tolerability in combination with a small number of side effects;
soft, balanced nature of the action, uniform influence on all components of depressive affect (anxiety, melancholy, apathy);
effects on anxiety-depressive, depressive-phobic and depressive- hypochondriac states;
ease of use (once a day, there is no need to select the optimal dose);
lack of severe sedation , which allows you to maintain the usual rhythm of life and social activity.
In addition, Zoloft treatment of depressive disorders allows not only to eliminate the clinical symptoms, but also to restore the patient's quality of life - psychological comfort, social relationships, and work.
0 Comments
Reply